
Becoming an ECMO Specialist
Who Is Better Prepared for ECMO: A Nurse or a Respiratory Therapist?

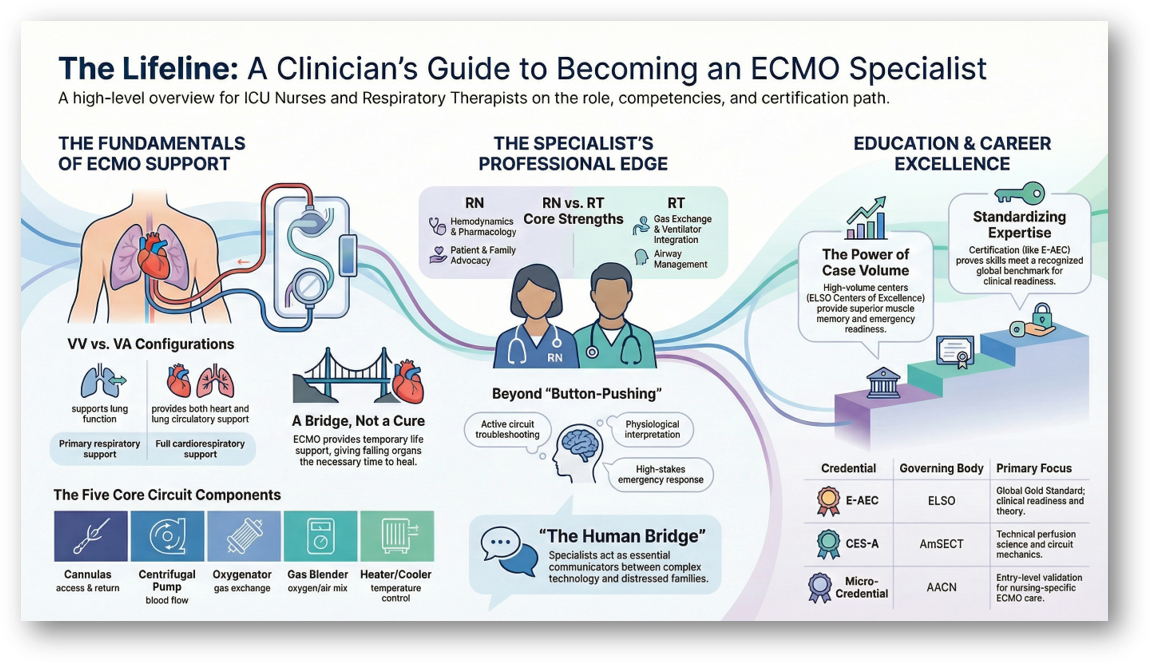
Both nursing and respiratory therapy backgrounds provide distinct, highly valuable skill sets that uniquely prepare clinicians for the role of an ECMO Specialist. While both professions work in high-stakes critical care environments, they approach the therapy from different foundational strengths.
The Nurse’s Advantage: Holistic Patient Management. Critical care nurses excel at comprehensive patient management and bring a distinct advantage in treating the body as a whole system. Their unique contributions include:
Holistic Assessment: Nurses are trained to perform thorough head-to-toe assessments, allowing them to notice subtle changes, such as decreased urine output, mottling, or pupillary asymmetry, that may indicate underlying circuit or perfusion issues.
Complex Pharmacology: ECMO patients require careful combinations of sedatives, paralytics, vasopressors, and anticoagulants. Nurses already understand how these complex medications interact, how to safely titrate them, and how to monitor for side effects.
Line and Wound Care: Nurses are highly experienced with invasive lines (central lines, arterial lines, chest tubes) and sterile techniques. This translates directly to monitoring ECMO cannulas, securing sites, preventing infection, and managing localized bleeding.
Hemodynamic Management: Nurses, particularly those from cardiac ICUs, are adept at walking the tightrope of balancing blood pressure and perfusion, which is crucial when managing circuit flow alongside a patient’s native cardiac function.
Care Plan Execution and Family Communication: Nurses are experts at integrating the multidisciplinary care plan, including nutrition, skin care, and mobility, and serve as a crucial, compassionate bridge for families who are overwhelmed by the ECMO machinery.
The Respiratory Therapist’s Edge: Mastering the Mechanics. Respiratory therapists (RTs) bring an unparalleled expertise in gas exchange and cardiopulmonary mechanics, which form the core of what ECMO actually does. Their unique contributions include:
Gas Exchange and ABG Mastery: RTs deal with gas exchange physiology daily. They can swiftly interpret arterial blood gas (ABG) panels, including pre-oxygenator and post-oxygenator gases, and immediately determine the appropriate interventions.
Sweep Gas Management: The tasks of adjusting sweep gas to clear carbon dioxide and adjusting FiO₂ to optimize oxygenation mirror what RTs already do with mechanical ventilators. This gives them a major head start in manipulating the ECMO circuit’s artificial lung.
Mechanical Ventilation and ECMO Integration: In VV ECMO, the goal is often to “rest” the lungs. RTs are uniquely skilled at balancing extracorporeal support and protective mechanical ventilation (e.g., low tidal volumes or minimal PEEP) to prevent lung trauma.
Oxygenator Troubleshooting: When a patient desaturates, RTs naturally follow a methodical sequence to diagnose the issue (e.g., checking gas flow, FiO₂, or looking for clotting), mirroring how they troubleshoot a deteriorating patient on a ventilator.
Ultimately, becoming an ECMO specialist requires both professions to bridge their knowledge gaps. Nurses must deepen their understanding of circuit physics and advanced gas exchange, while RTs must expand their scope to encompass total-body hemodynamics, broad-spectrum pharmacology, and comprehensive patient care.
Learn more
If you want more ECMO breakdowns like this, subscribe to this newsletter, ECMO 143: AI-Assisted Journey. I’ll keep sharing what I’m learning along the way.
You can also use my free Custom GPT, AI ECMO Educator.
An evidence-based ECMO and ECPR educator for ICU clinicians and trainees, covering physiology, cannulation, anticoagulation, circuit management, and troubleshooting.
Sources include ELSO, PubMed, AmSECT, and leading centers. Version 5.2 (2/21/26) | Supports 50+ languages.