


Recently, I heard about a patient with SAM, systolic anterior motion of the mitral valve. I had never even heard of it, much less understood what it meant at the bedside. Even after someone explained it, I still had questions. So after a long shift, I started doing what I often do now: AI-assisted research, checking what I found against ECMO references, and trying to translate the concept into plain language.
SAM itself is a very specific cardiac problem, and this article is not meant to be a deep dive into SAM. What caught my attention was something bigger. It reminded me that adult ECMO patients often arrive with diagnoses, physiology, and clinical pathways that I do not fully understand yet. I may know the general ECMO language, bridge to recovery, bridge to transplant, bridge to device, bridge to decision, but those phrases can become vague if I do not stop and ask a more basic question.
ECMO Is a Bridge, but the Failure Comes First
That question helped me think less in terms of disease lists and more in terms of failed physiology. A patient does not go on ECMO simply because they have pneumonia, myocarditis, pulmonary embolism, cardiogenic shock, or ARDS. Many patients have those diagnoses and never need ECMO. The bigger issue is that one or more parts of oxygen delivery have failed badly enough that conventional support is no longer enough, or the support required to keep the patient alive is becoming harmful.
Here is the simple framework I am using:
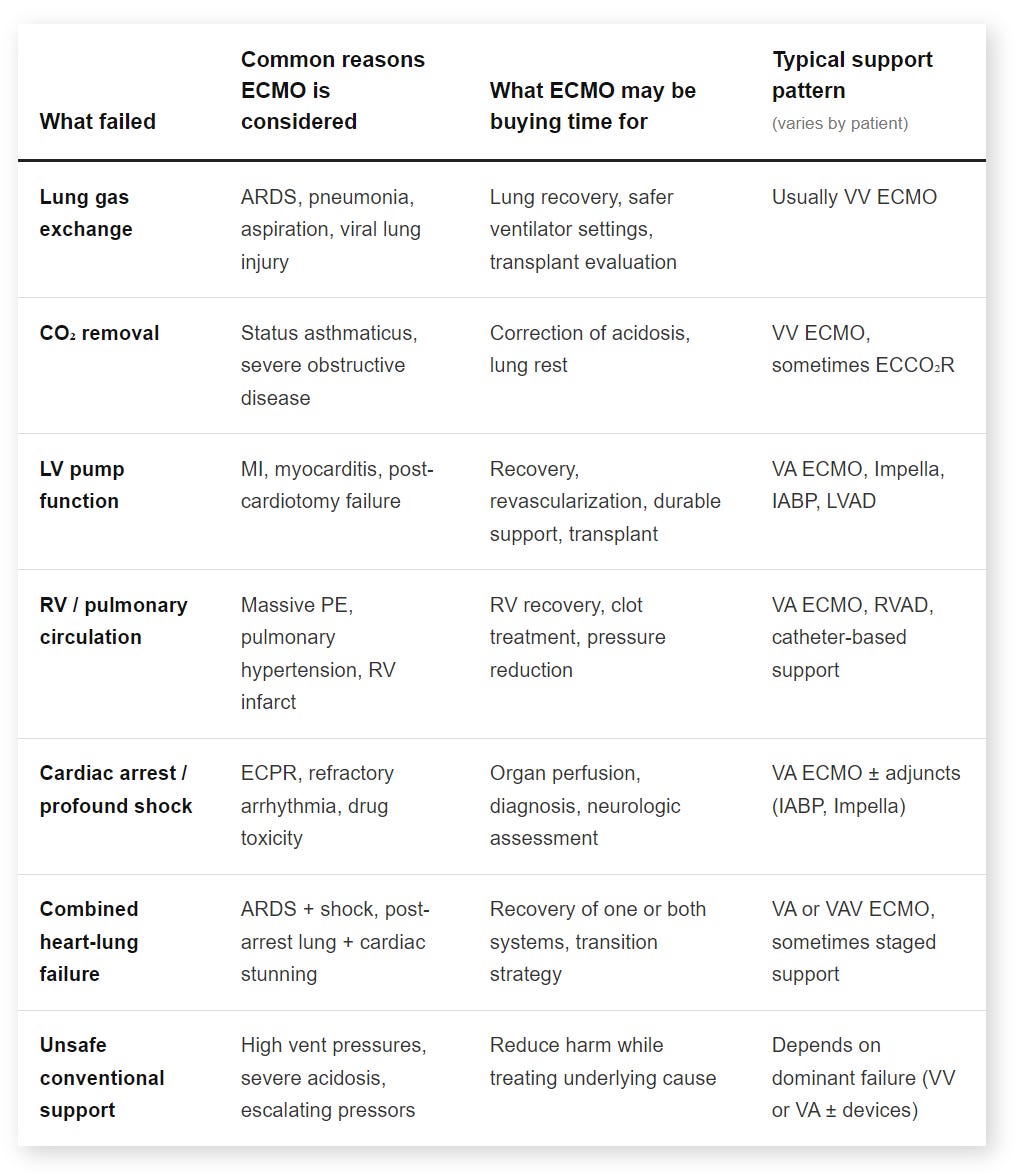
Lung Failure: When Gas Exchange Is the Problem
For lung failure, the main issue is gas exchange. The heart may still be able to pump blood forward, but the lungs cannot oxygenate, remove CO2, or do either without injurious ventilator settings. This is the world where VV ECMO usually makes sense. VV ECMO does not directly support blood pressure or cardiac output. It supports gas exchange while the patient’s own heart continues to move blood through the body. That distinction matters because low oxygen is not the only question. The better question is whether the lungs are the main failed system and whether the native heart can still deliver blood forward.
Pump Failure: When Oxygenated Blood Cannot Reach the Organs
For pump failure, the problem is different. The blood may contain oxygen, but the heart cannot move enough of it to the organs. This is where cardiogenic shock becomes more than a label. The real issue is oxygen delivery: cardiac output, perfusion pressure, lactate, urine output, mental status, and end-organ function. VA ECMO can provide systemic perfusion while the team treats the cause or decides the next step. Sometimes the heart recovers after myocarditis, myocardial stunning, revascularization, or surgery. Sometimes it does not, and the path becomes a temporary device, durable VAD, transplant evaluation, or a difficult bridge-to-decision conversation.
Right Heart Failure: When Blood Cannot Move Through the Lungs
Right-heart and pulmonary vascular failure deserve their own mental category. Heart failure does not always mean left-heart failure. In massive pulmonary embolism, severe pulmonary hypertension, RV infarct, or acute RV failure, the right ventricle may not be able to move blood through the pulmonary circulation. That can lead to shock, poor LV filling, hypoxemia, high venous pressures, and systemic hypoperfusion. The key question is not simply whether the patient has “heart failure,” but whether the right heart can move blood through the lungs.
Combined Failure: When the Boxes Stop Being Clean
Some patients do not fit cleanly into one box. They may have severe ARDS with septic cardiomyopathy, post-arrest aspiration with myocardial stunning, or VA ECMO physiology complicated by differential hypoxia. This is where VAV ECMO or another hybrid strategy may enter the conversation. I do not want to turn this article into a cannulation discussion, but the principle is important: the mode should follow the physiology. VV helps gas exchange, VA helps systemic perfusion, and VAV may be considered when both problems need support.
When Conventional Support Becomes Too Harmful
The other piece I am learning is that ECMO is sometimes considered not only because the patient’s numbers are bad, but because the support needed to keep those numbers acceptable is becoming dangerous. High ventilator pressures can worsen lung injury. Severe acidosis can worsen hemodynamics. Escalating pressors may preserve a blood pressure while tissue perfusion continues to fail. ECMO adds real risk, so it has to create a path that did not exist before.
That path might be recovery. It might be transplant. It might be a device. It might be an intervention. Sometimes it is simply time to understand whether recovery is possible.
The Question I Want to Ask Better
The SAM case reminded me how much I still have to learn, but it also helped me ask a better question. When I hear that a patient is going on ECMO, I do not only want to ask, “What diagnosis do they have?” I want to ask, “What physiology failed, and what are we trying to buy time for?”
That may be the clearer way to understand ECMO as a bridge. Not just bridge to recovery, but bridge from a specific physiologic failure toward a specific possible next step.
Learn more
You are reading ECMO 143: AI-Assisted Journey on LifeSupport.training, where I share practical ECMO articles, study notes, and tools for clinicians learning extracorporeal life support.
I also built AI ECMO Educator, a free-to-use tool that provides evidence-based ECMO and ECPR guidance for ICU clinicians and trainees. It covers topics such as physiology, cannulation, anticoagulation, circuit management, and troubleshooting, drawing from sources including ELSO, PubMed, AmSECT, and leading ECMO centers.
Disclaimer
This content is for educational purposes only. It does not replace clinical judgment, institutional protocols, or consultation with your ECMO team.