

I understood the basics of hemolysis on ECMO. Watch for rising plasma-free hemoglobin, clots, and high negative inlet pressures.
What I had not fully worked through were the consequences. How free hemoglobin contributes to kidney injury, vasoconstriction, and oxidative stress. Or how to interpret labs like haptoglobin in a meaningful way.
So I did an AI-assisted deep dive and turned it into a practical breakdown for the bedside.
What is hemolysis?
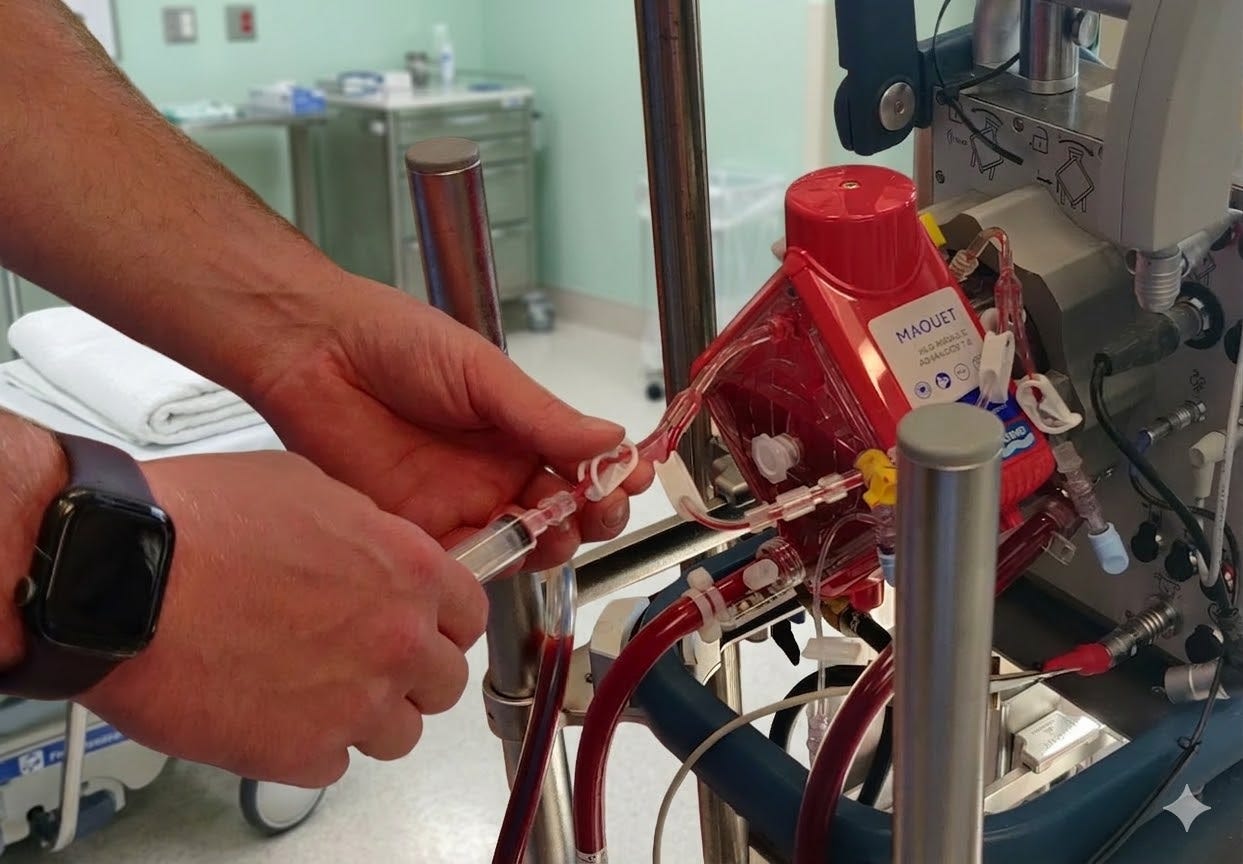
Hemolysis is the destruction of red blood cells. On ECMO, it usually means the circuit is stressing the blood due to suction, turbulence, or clot.
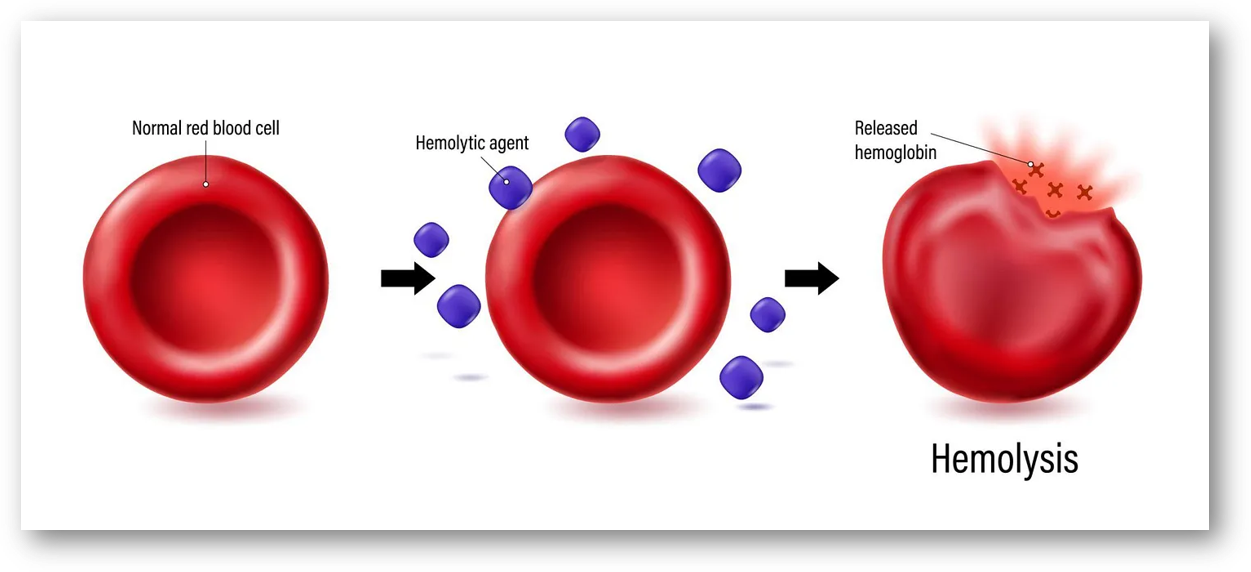
When red blood cells rupture, hemoglobin is released into the plasma. This is intravascular hemolysis.
A small amount of hemolysis can occur even in a normal circuit. The concern is when it increases or begins trending upward.
Why it matters
Hemolysis is often the first warning that the ECMO circuit is developing a mechanical problem.
On ECMO, hemolysis is usually circuit-related, not just patient-related. It can point to high shear stress, very negative drainage pressure, suction events, fibrin deposition, pump thrombosis, or oxygenator clot burden before the situation becomes a full circuit emergency.
Free hemoglobin is directly harmful.
Once hemoglobin is released into plasma, it is no longer contained. Free hemoglobin, heme, and free iron contribute to oxidative injury, deplete nitric oxide, promote vasoconstriction, and can lead to renal tubular injury and abnormal coagulation. This can progress to organ dysfunction.
Hemolysis also reduces effective oxygen delivery.
Red blood cell destruction contributes to anemia, but more importantly, rising plasma-free hemoglobin is associated with worse clinical outcomes during ECLS. It reflects both a blood problem and a system problem.
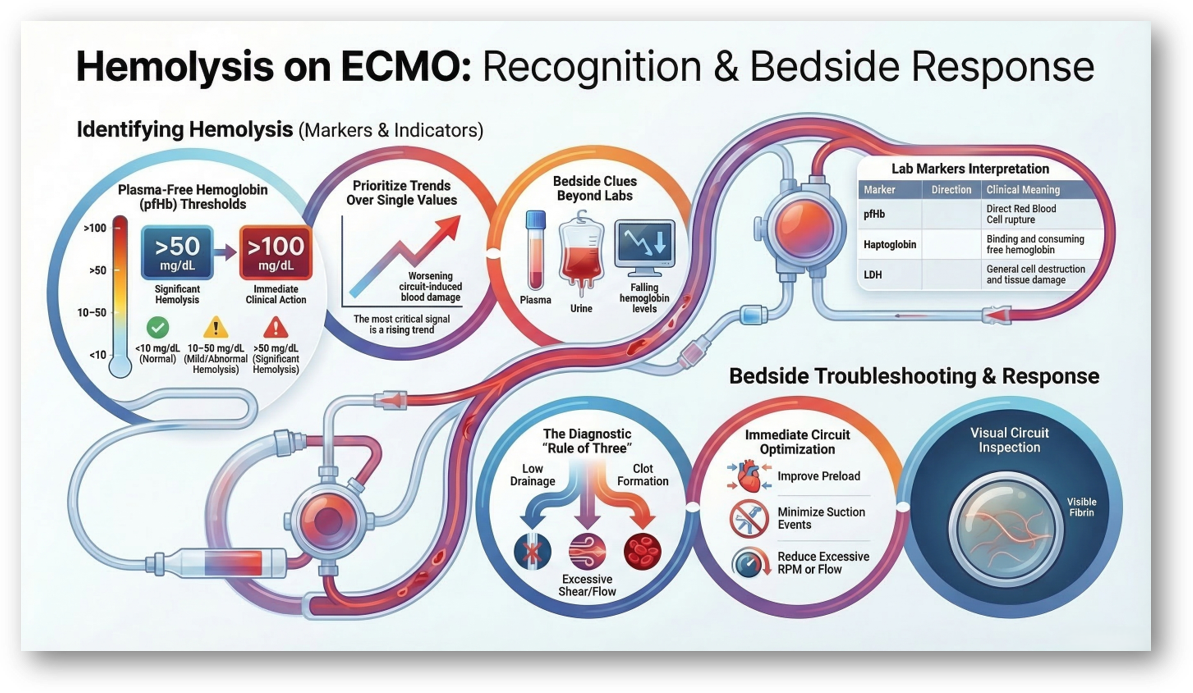
How to recognize hemolysis on ECMO
No single lab confirms hemolysis on its own. You need a pattern and a trend.
The most important question is not “is this abnormal?” but “is this getting worse?”
What to look for
Strongest indicator:
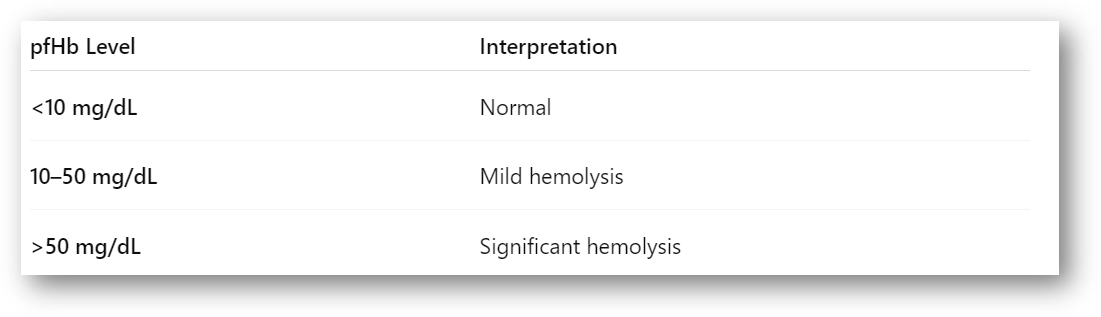
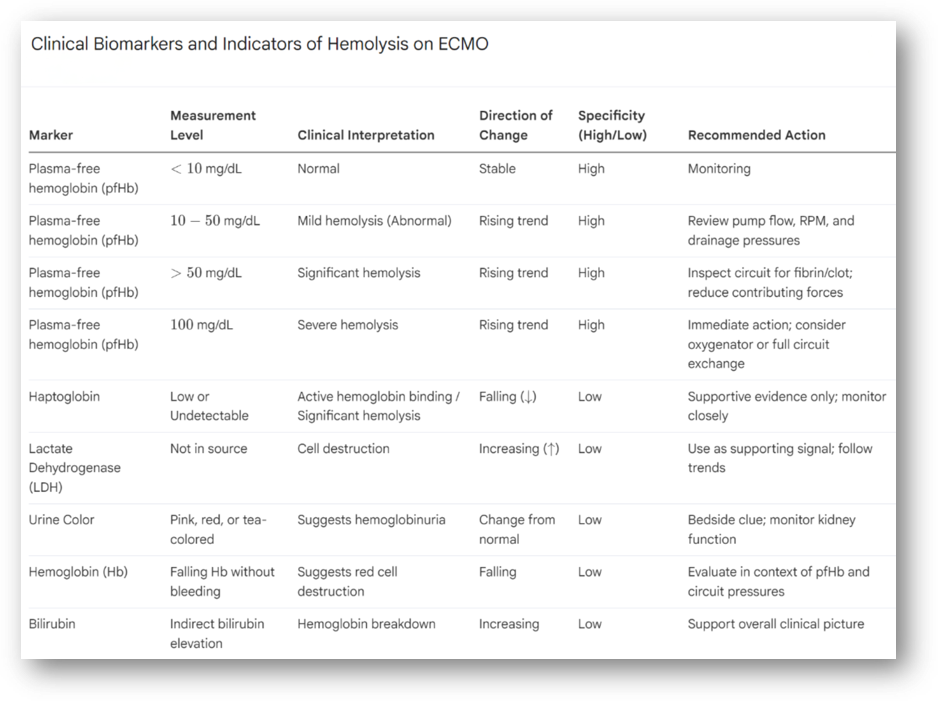
Plasma-free hemoglobin (pfHb)
This is the principal biomarker for intravascular hemolysis.
<10 mg/dL: Normal
10-50 mg/dL: abnormal in some studies
>50 mg/dL: widely used threshold for significant hemolysis
100 mg/dL: severe and should prompt immediate action
A rising trend is the most important signal
Supportive indicators:
These support the diagnosis but are not specific on their own.
Lactate Dehydrogenase (LDH)
LDH is released when cells break down.
It supports the diagnosis of hemolysis, but it is not specific. LDH also rises in shock, liver injury, and tissue damage.
Use LDH as a supporting signal, not a primary one.
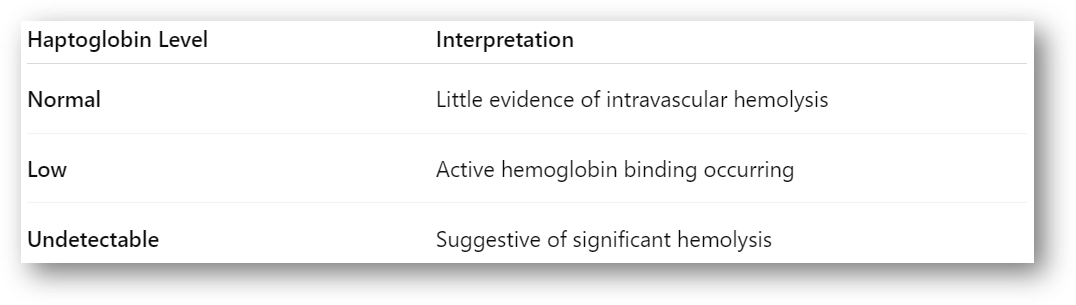
Haptoglobin
Haptoglobin binds free hemoglobin.
When hemolysis occurs, haptoglobin is consumed and levels fall.
Low or undetectable haptoglobin supports hemolysis, but it is unreliable in critically ill patients. Many ECMO patients already have low levels at baseline.
Think of it as supportive evidence only.
Bilirubin
Indirect bilirubin may rise as hemoglobin is broken down.
This is a slower marker and not specific. It helps support the overall picture but should not drive decisions on its own.
Hemoglobin (Hb)
A falling hemoglobin can suggest hemolysis, but it is not specific.
On ECMO, hemoglobin can drop for several reasons: bleeding, dilution, or lab draws.
If hemoglobin is falling and plasma-free hemoglobin is rising, that combination is more concerning.
Hemoglobinuria
Pink, red, or tea-colored urine can suggest hemoglobinuria.
This is a useful bedside clue but not diagnostic on its own.
Falling hemoglobin without bleeding
Suggests red cell destruction but requires context.
Circuit clues
These increase suspicion for circuit-related hemolysis:
Very negative drainage pressure
Suction events or chatter
Rising transmembrane pressure (>60 mmHg)
Fibrin deposition or visible clot
Worsening oxygenator gas transfer
Why hemolysis happens
Most causes fall into three categories:
1. Drainage problems
High negative inlet pressure
Suction events
Hypovolemia
Cannula malposition
2. Flow and shear
High RPM
Excessive flow for cannula size
Turbulent flow
3. Circuit or device issues
Oxygenator clot or fibrin buildup
Pump head thrombosis
Tubing kinks or obstruction
4. Other mechanical support devices
Hemolysis is not limited to ECMO.
Devices like Impella can also contribute due to shear stress, especially with high support levels, suction events, or malposition.
In patients on combined support (ECMO + Impella), both systems should be evaluated.
What to do at the bedside
Start with one question:
Why is this circuit or device damaging blood?
1. Assume the circuit until proven otherwise
Review pump flow, RPM, drainage pressures, and recent suction events.
Hemolysis worsens with high flow, high shear, poor preload, and unstable drainage.
2. Inspect the circuit
Use a bright light. Look at the oxygenator and tubing for fibrin or clot.
If there is visible clot, rising pressures, or worsening gas exchange, treat that as part of the problem.
3. Reduce contributing forces
Improve preload if appropriate
Minimize suction events
Reduce excessive flow or RPM
Stabilize drainage conditions
4. Escalate early if the trend is worsening
If hemolysis is severe, rising, or associated with thrombosis:
Consider oxygenator exchange
Consider full circuit exchange
5. Evaluate other devices
If present:
Check Impella position
Reduce support level if appropriate
Address suction or malposition
6. Monitor the patient closely
Follow:
Plasma-free hemoglobin
Kidney function
Urine color
Hemoglobin trend
LDH and bilirubin
Hemolysis can quickly shift from a circuit issue to a patient injury issue.
The bedside framework
When plasma-free hemoglobin is rising, narrow it down:
Too little drainage
Too much shear
Or clot forming
Most problems fall into one of these three.
Final thought
Hemolysis is one of the clearest signals that the ECMO circuit or support device may be harming the patient.
If plasma-free hemoglobin is rising, something is wrong.
Find it early. Fix it early.
Learn more
If you want more ECMO breakdowns like this, subscribe to ECMO 143: AI-Assisted Journey. I’ll keep sharing what I’m learning along the way.
You can also use my free Custom GPT, AI ECMO Educator.
An evidence-based ECMO and ECPR educator for ICU clinicians and trainees, covering physiology, cannulation, anticoagulation, circuit management, and troubleshooting.
Sources include ELSO, PubMed, AmSECT, and leading centers.
Version 5.2 (2/21/26) | Supports 50+ languages.
Disclaimer
This content is for educational purposes only and does not replace clinical judgment, institutional protocols, or consultation with your ECMO team.