


Despite my background in teaching Advanced Cardiovascular Life Support (ACLS), I'm new to Postoperative Cardiac Surgery Protocols (PCS), also referred to as Cardiac Advanced Life Support (CALS) in some settings. These protocols, or very similar ones, are endorsed by organizations like the Society of Thoracic Surgeons (STS), the European Resuscitation Council (ERC), and the European Association of Cardio-Thoracic Surgery (EACTS). Designed specifically for managing cardiac arrests following cardiac surgeries, PCS/CALS shares some common ground with ACLS but is tailored to the unique needs of surgical patients, addressing challenges like the high risk of graft injury and other surgical complications. This article dives into PCS/CALS, explaining how it differs from ACLS and the specialized roles essential for optimal patient outcomes.
Deciding Between PCS/CALS and ACLS Protocols
The choice between using PCS/CALS or ACLS depends on several factors, including the patient’s recent surgical history, the location of the cardiac arrest, and available resources:
Patient History: If a patient has recently undergone cardiac surgery, PCS/CALS is generally preferred over ACLS due to specific considerations like avoiding high-dose adrenaline and prioritizing internal cardiac massage.
Location of Arrest: PCS/CALS protocols are usually applied in specialized cardiac surgical units or ICUs where the necessary tools (such as a resternotomy kit) and trained staff are readily available. However, if an arrest occurs outside these settings, staff may initiate ACLS first and transfer the patient to a specialized unit to continue with PCS/CALS protocols as needed.
Medical Team Involvement: Senior medical staff, including ICU leads or cardiothoracic surgeons, often decide based on the patient’s condition. This guidance is especially important in complex cases involving additional surgical complications or time-sensitive factors.
Hospital Protocols: Many hospitals have specific guidelines for when PCS/CALS should be applied, helping standardize care and optimize outcomes for postoperative cardiac patients.
Understanding PCS: Specifically for Postoperative Cardiac Surgery Patients
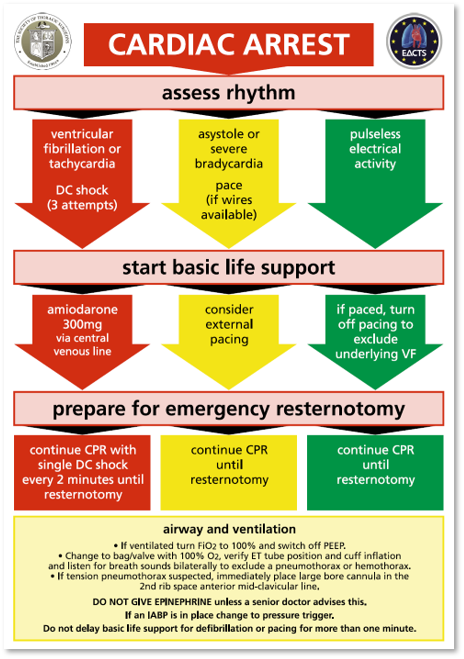
PCS/CALS protocols are designed to address the unique needs of cardiac arrest patients who have recently undergone surgery. Although cardiac arrest incidence after cardiac surgery is low, it often involves reversible causes such as ventricular fibrillation (VF), cardiac tamponade, or hypovolemia. PCS/CALS differs from ACLS by prioritizing rapid defibrillation, pacing, and, if necessary, emergency resternotomy (surgical reopening of the chest, specifically along the sternotomy incision made during the initial cardiac surgery).
Key Components of PCS/CALS:
Three-Stacked Shocks for Ventricular Fibrillation (VF): For VF, PCS/CALS uses three rapid defibrillation shocks before external compressions to protect surgical sites.
Avoidance of High-Dose Adrenaline: In PCS/CALS, adrenaline is minimized or avoided to prevent sudden blood pressure increases that could harm grafts or surgical repairs.
Early Resternotomy: If initial efforts fail, an emergency resternotomy within five minutes is advised, allowing internal cardiac massage, which can significantly improve patient outcomes.
PCS/CALS has become widely adopted in cardiac surgical centers as an essential protocol for postoperative care, improving survival outcomes by addressing these specific needs.
Team Roles in PCS Protocols
In PCS/CALS, every second counts, and specific roles within the team are critical. Each team member has responsibilities that contribute to the rapid, specialized care required in these cases. Below is an illustration of the ideal placement of team members around the patient in a resuscitation room, followed by a summary of the roles:


These well-defined roles improve the team’s efficiency and readiness for potential interventions like internal defibrillation or resternotomy, setting PCS/CALS apart from the more general approach of ACLS.
Differences Between PCS and ACLS Protocols
While ACLS is an invaluable guideline for general cardiac arrests, PCS takes a different path to address the specific needs of postoperative cardiac patients. Here’s a side-by-side comparison of some core differences:

That all said:
Learning PCS/CALS has opened up a new perspective on cardiac arrest management for me, highlighting the need for specialized protocols in postoperative cardiac surgery patients. While ACLS remains foundational for most cardiac arrests, PCS offers a more tailored approach that considers the risks of injury to surgical sites, the need for rapid defibrillation or pacing, and even the possibility of resternotomy. For those of us who work with post-cardiac surgery patients, adopting PCS/CALS practices can make a life-saving difference.
References:
Brand J, McDonald A, Dunning J. Management of cardiac arrest following cardiac surgery. BJA Education. 2018 Jan;18(1):16-22. doi: 10.1016/j.bjae.2017.11.002.
Dunning J, Levine A, Ley J, et al. The Society of Thoracic Surgeons expert consensus for the resuscitation of patients who arrest after cardiac surgery. Ann Thorac Surg. 2017 Apr 1;103(4):1005-20. doi: 10.1016/j.athoracsur.2016.12.081.
Rousou JA, Engelman RM, Flack JE, Deaton DW, Owen SG. Emergency cardiopulmonary bypass in the cardiac surgical unit can be a lifesaving measure in postoperative cardiac arrest. Circulation. 1994 Sep;90(4 Pt 2)
2020 American Heart Association Advanced Cardiovascular Life Support Provider Manual.
Join the ECMO 143 Learning Journey
Note: This article is intended for educational purposes only. It should not be used as a substitute for professional medical advice or guidance. Always consult with qualified healthcare professionals for clinical decisions and patient care.
Other Links:
https://bit.ly/ecmo143-youtube
https://bit.ly/ecmo143-company
Acknowledgments:
Here is a list of tools and resources that assisted in creating this article and others. I developed three custom GPTs for specialized research: AI ECMO Expert, ECMO Specialist Handover Practice, and Micro Definitions (MD-GPT). These tools were instrumental in gathering and analyzing information from key sources.
Special thanks to the AI platforms and tools that facilitated this research:
GPT-4o/o1, Claude 3.5 Sonnet/Opus, Perplexity
Grammarly for editorial and proofreading assistance
Leonardo AI, DALL-E3 AI Image Generator, Microsoft Designer, and Adobe Express for generating images and visual content