
When Heparin Turns on You: Understanding HIT and the Role of Bivalirudin in ECMO
🗓️ This is an advance release from my LinkedIn newsletter ECMO 143. Full article goes live there at 7:30 AM tomorrow.


Key Points (Before You Dive In)
HIT is a prothrombotic immune complication triggered by heparin.
Use the 4T score to assess likelihood of HIT before testing.
Confirm with PF4 ELISA and SRA if HIT is suspected.
If HIT is likely, stop heparin and switch to a direct thrombin inhibitor like bivalirudin.
Match the anticoagulant to the right test: Anti-Xa for heparin, aPTT for bivalirudin/argatroban.
Monitor closely, especially in unstable ECMO patients.
Introduction
I remember the first time I heard someone say, “The patient’s platelets just dropped by half—could be HIT.” At the time, I nodded, pretending to understand. I had no idea what they meant. It wasn’t covered in any of the ECMO training I’d gone through. It wasn’t until later that I realized how dangerous—and how commonly overlooked—this complication is.
What is HIT?
Heparin-Induced Thrombocytopenia (HIT) is a life-threatening immune complication of heparin therapy. HIT occurs when antibodies form against complexes of heparin and platelet factor 4 (PF4), leading to platelet activation, thrombocytopenia, and an increased risk of thromboembolic events such as DVT, stroke, and ECMO circuit clotting.
This prothrombotic state—despite falling platelets—is one of the most dangerous complications of anticoagulation on ECMO and must not be confused with typical circuit-related thrombocytopenia.
According to the ELSO Red Book, HIT is more common in adult VA ECMO patients, and its diagnosis should trigger immediate anticoagulant reassessment. The ECMO Specialist Training Manual further highlights that circuit thrombus or oxygenator failure should always prompt a review of the patient’s platelet count and coagulation profile.
Diagnosing HIT: The 4T Score
The 4T Score is a clinical tool to estimate the pretest probability of HIT and guide further testing. It includes four components:
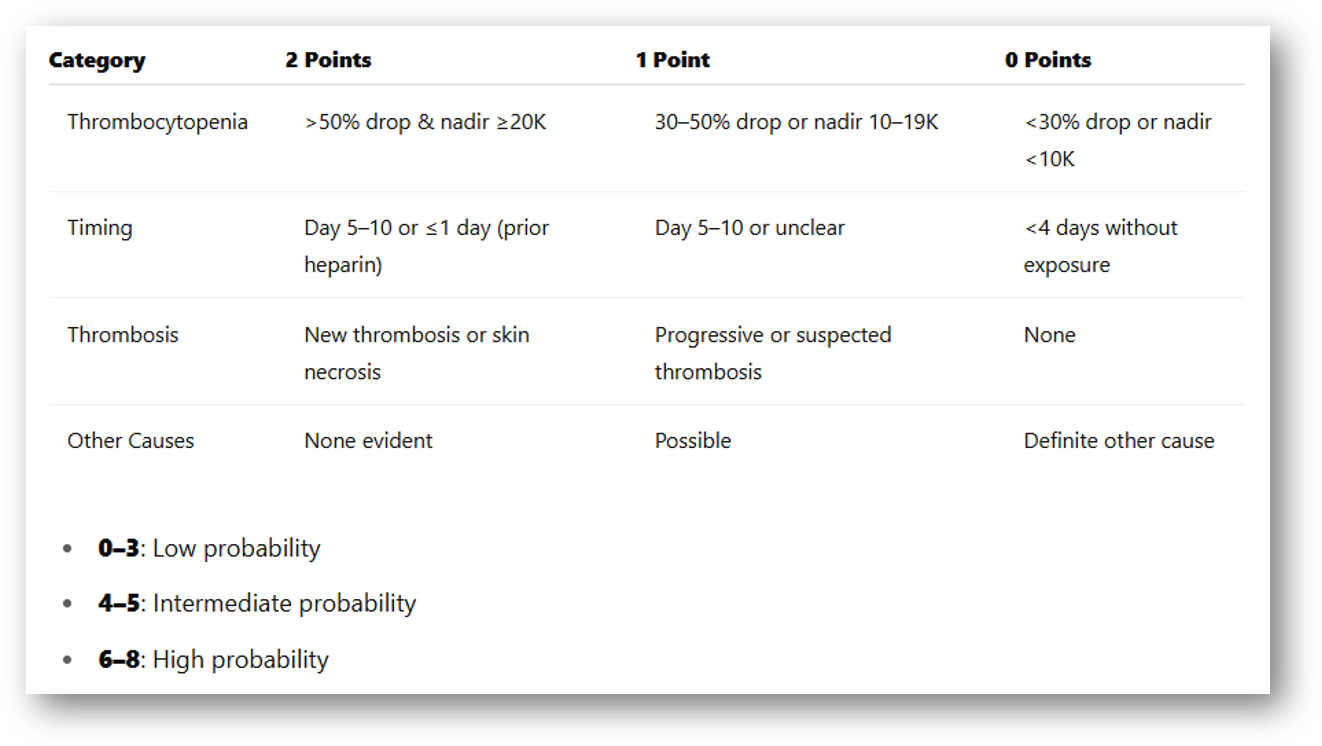
In ECMO, a 50% platelet drop occurring on or after Day 5, especially with new thrombosis or oxygenator dysfunction, should never be dismissed as routine. It demands immediate investigation.
Confirmatory Testing
PF4 ELISA: High sensitivity but prone to false positives; useful for screening.
SRA (Serotonin Release Assay): The gold standard test for HIT; confirms actual platelet-activating antibodies.
ELSO and The ECMO Book recommend using both the 4T Score and functional assays to improve diagnostic accuracy.
Case Study: HIT in ECMO
Patient: 62-year-old male on VA ECMO for cardiogenic shock
Day 5: Platelets drop from 210k to 95k
Findings: New leg swelling; ultrasound confirms DVT
4T Score: 7/8 (High probability)
Labs: Positive PF4 ELISA; HIT confirmed by SRA
Management: Heparin discontinued; initiated bivalirudin
Outcome: Platelet count rebounded; no new thrombosis
Why Bivalirudin?
Bivalirudin is a direct thrombin inhibitor preferred in ECMO patients with HIT. Compared to heparin:
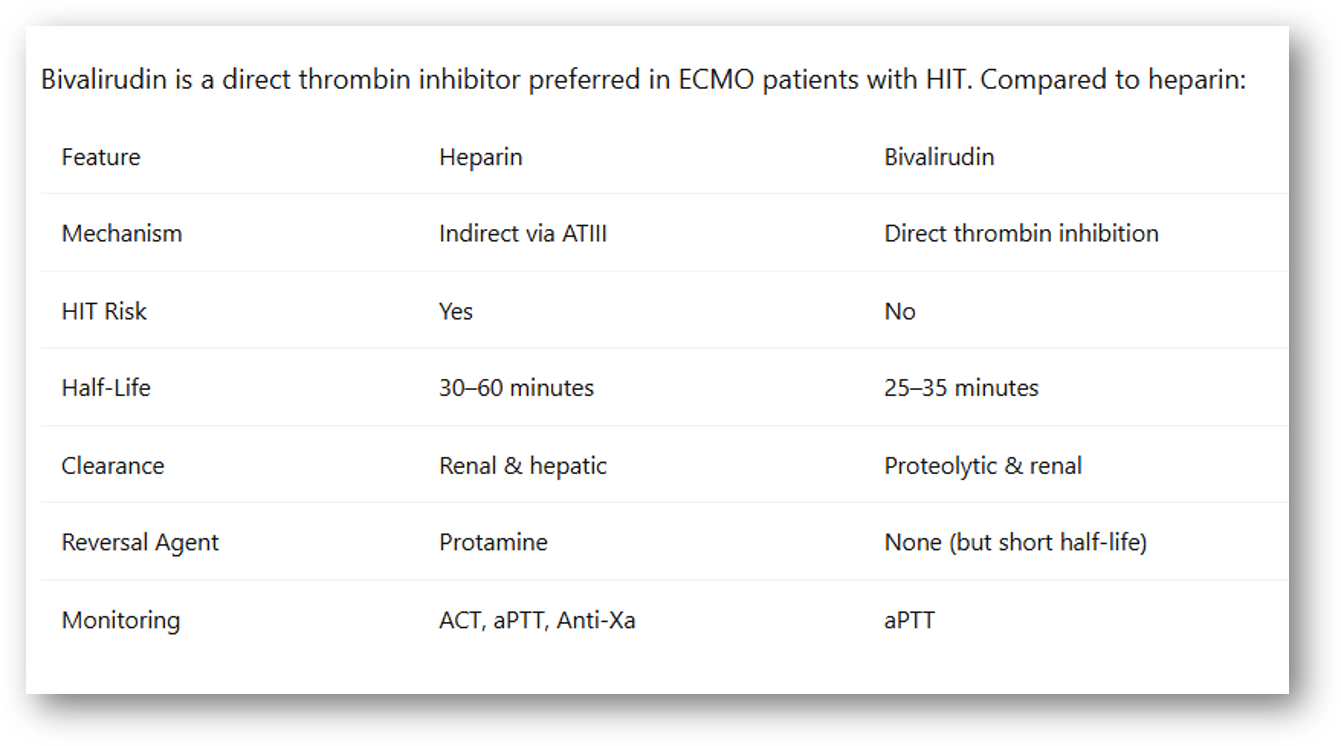
Bivalirudin’s stable pharmacokinetics and non-dependence on antithrombin make it ideal for ECMO, especially in unstable patients or when HIT is confirmed or suspected.
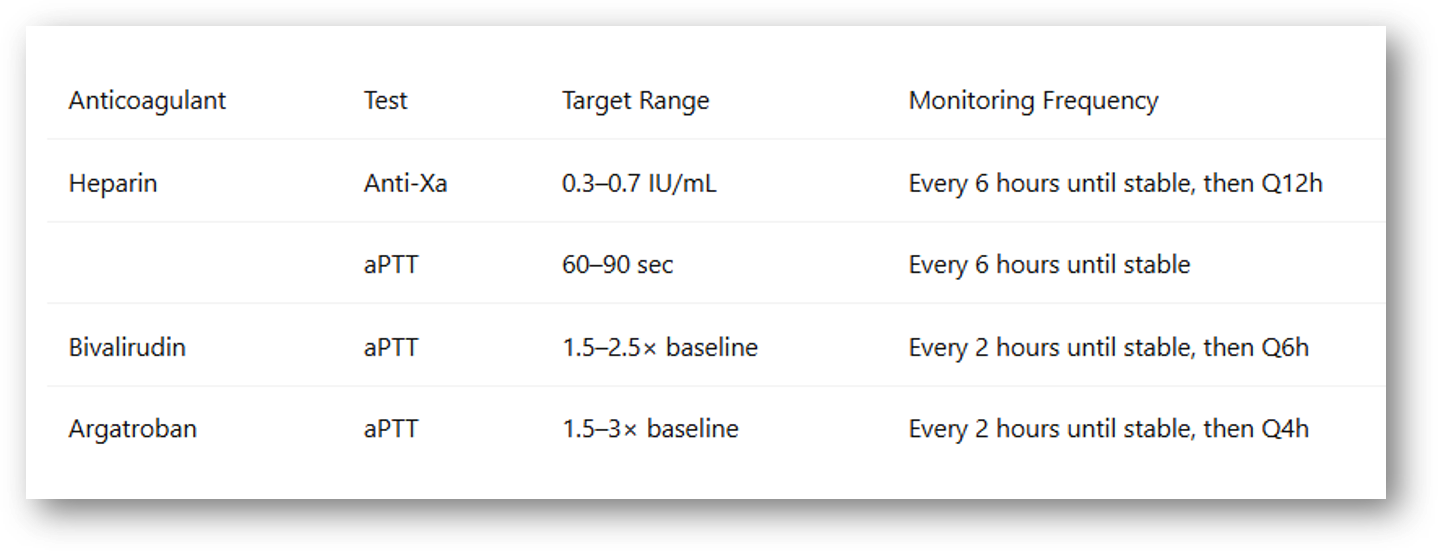
Monitoring Frequency by Anticoagulant
Takeaway for ECMO Specialists
If your patient’s platelets drop by >50% on Day 5–10 of ECMO—and you see thrombus in the circuit or a failing oxygenator—don’t write it off. Calculate the 4T score, confirm with PF4 ELISA and SRA, and change your anticoagulant early if HIT is likely.
Bivalirudin is often the best alternative, but it must be paired with aPTT monitoring—and frequently reassessed during instability. Remember:
Heparin → Anti-Xa (or aPTT)
Bivalirudin / Argatroban → aPTT
Match the drug to the test. Monitor wisely.
AI plays a significant role in how I research, understand, and communicate complex ECMO topics. From analyzing source materials to organizing ideas and generating podcast outlines, AI helps me stay curious and keep learning—so I can keep sharing.
Check out my websites:
lifesupport.training for ECMO and other professionals
ecmo.life for patients and loved ones
Occasional podcasts are on YouTube
Latest real time ECMO News on my ECMO143 UpToDate X Channel
Disclaimer
This article is for educational purposes only and reflects my understanding and interpretation of available guidelines, literature, and bedside learning. It does not constitute medical advice or represent institutional protocols. Always consult your ECMO team and local policies when making clinical decisions.
References
Extracorporeal Life Support Organization (ELSO). Extracorporeal Life Support: The ELSO Red Book. 6th ed. Ann Arbor, MI; 2023.
ELSO. ECMO Specialist Training Manual. 4th ed. Ann Arbor, MI; 2022.
DellaVolpe J. The ECMO Book. San Antonio, TX: The Institute for Extracorporeal Life Support; 2024.
Zhao Y, et al. Bivalirudin Anticoagulation in ECMO: Monitoring and Management. Crit Care Med. 2021.
Nguyen TP, et al. Heparin Monitoring in ECMO: aPTT vs. Anti-Xa. J Cardiothorac Vasc Anesth. 2021.
Renou A, et al. HIT Risk Stratification Using Modified 4T in ECMO. Intensive Care Med. 2020.
Frontiers in Pharmacology. Bivalirudin Anticoagulation Guidelines. 2023.
Repost, Comment & Subscribe
What stood out to you in this article? I’d love to hear your take. Join the ECMO 143 learning journey: real-world ECMO education with AI-powered insight, bedside clarity, and no fluff.